Fronto-temporal degeneration is primarily manifested in concurrent or successive behavioural and language disorders. The progression to generalized dementia is more or less rapid.
Symptoms of fronto temporal dementia (FTD)
The patient’s condition deteriorates over the years. The symptoms of FTD are highly variable from patient to patient, in their manifestations as well as in their order of onset and progression.
In the early stages of FTD, behavioural disorders are discrete and may evoke the effects of fatigue, stress or depression.
The first disorders are often mental fatigue or apathy, loss of motivation, indifference to emotions and others, even those close to them, or loss of envy.
A second, more visible type of symptoms are behavioural disorders such as severe disinhibition and an inability to observe social codes – inappropriate thinking, disobeying rules when driving or in public spaces. It can also be agitation or aggression, running away or the development of obsessions. Patients may act strangely by, for example, continually repeating the same actions, fixating on certain habits or objects and becoming compulsive collectors. Some patients may have an irrepressible need to move, such as walking several kilometres for no specific purpose. Lack of patience and excessive irritability are sometimes observed.
Changes in eating behaviour are also present in many patients, such as gluttony – eating excessively and precipitously – or phases of bulimia or anorexia.
In some cases patients may neglect themselves, with a loss of personal hygiene and clothing.
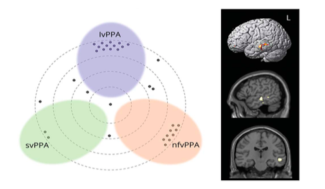
Language disorders in FTD can take different forms and affect either syntax (meaning of words) or fluence:
- Aphasis is a loss of speech manifested by difficulty in pronouncing words, loss of vocabulary or, at later stages, a complete inability to speak. However, the understanding of words is preserved.
- Semantic dementia, in which understanding is affected rather than pronunciation, occurs when the left part of the brain is more affected. Patients are unable to name objects (anomic aphasia) or recognize the faces of loved ones (prosopagnosia).
Other disorders appear later in particular confusion, disturbances of judgment, planning with an impossibility for the patient to achieve simple things.
Motor symptoms may appear at an advanced stage of the disease, such as rigidity of movement or walking disorders. FTD is first suspected through the testimony of relatives who report changes in a parent’s behavior, personality change, or language difficulties.
Additional examinations confirm the diagnosis of FDT. First of all, neuropsychological tests, which assess patients’ reasoning, judgment, attention and memory skills. Brain imaging tests, such as MRI or scanner, show atrophy of the frontal and temporal regions. Biological examinations, lumbar puncture or electroencephalogram may exclude other pathologies with similar symptoms.
In the case of familial genetic forms, about 50% of cases may be referred for genetic counselling and analysis to identify the mutation causing the disease.
At Paris Brain Institute
An important goal of research at the Brain Institute and IM2A is to improve patient diagnosis to detect disease earlier and limit wandering. FTD can be confused with several diseases depending on their stage, such as mood disorders (depression, bipolar disorder) or anxiety disorders (obsessive compulsive disorder), or Alzheimer’s disease.
Isabelle Le Ber and Paola Caroppo, in collaboration with the neuroimaging teams and the Centre for Clinical Investigation at Paris Brain Institute, have identified, using state-of-the-art brain imaging techniques, a very limited region of the brain involved in language comprehension, in the ability to interact with others and to recognize facial emotions (altered in patients with FTD), which may be the site of the first brain lesions in one form or another. Genetics of FTD. This major discovery enabled us to pinpoint the site of biological mechanisms, in particular neuronal death, even before the onset of clinical symptoms.
Patients with fronto-temporal dementia (FTD) are unable to categorize objects. By studying patients with lesions of the frontal cortex, the researchers of the team “FRONTLAB: Functions and dysfunctions of frontal systems” led by Dr. Richard Lévy have shown that categorization within the brain involves different functions, on the one hand the ability to gather information and on the other hand the ability to abstract. Both mechanisms depend on specific regions within the frontal lobes. This study paves the way for the use of concept training tests as a diagnostic tool for FTD.
A study by Marc Teichmann and Carole Azuar of Prof. Richard LEVY’s team, at Paris Brain Institute and at the Pitié-Salpêtrière-APHP hospital, shows that moral emotions, such as admiration, shame or pity, are particularly affected in patients with fronto-temporal degeneration. The results pave the way for early, sensitive and specific diagnosis of patients with FTD.