With longer life expectancies and the biological mechanisms at the origin of neurodegenerative diseases becoming increasingly complex, it is now estimated that, in France in 2020, 1.3 million people were affected by Alzheimer’s disease.
Today, more than 900,000 people are suffering from this disease, with 225,000 new cases each year. It affects 1 in every 20 people aged over 65, and more than 1 in 4 people after over 85.
-
1,2 million de personnes touchées en France
-
60 % des personnes touchées sont des femmes
-

30 000 personnes de moins de 60 ans sont touchées en France (source Inserm)
Alzheimer’s disease is the most common neurodegenerative disease in older people. The increase in average life expectancy, linked to healthier lifestyles, partly explains the increase in the number of people affected by this disease. Today, it is estimated that 900,000 suffer from Alzheimer-type dementia in France alone, with 35 million patients worldwide. Although onset of Alzheimer’s before the age of 65 is rare (0.5%), its incidence rises to between 2% and 4% after that age. It then rises proportionally with age, to reach over 15% by the age of 80. This disease increasingly affects women (1 in 4 women and 1 in 5 men over 85).
Biological mechanisms and causes of Alzheimer’s disease
Hereditary or ‘familial’ forms of Alzheimer’s disease are very rare, and account for less than 1% of cases. Onset occurs before the age of 60.
Symptoms sometimes appear as early as in a person’s thirties or forties. The disease is not hereditary in the strict sense, in 99% of cases, but genetic predisposing factors, so factors that increase the risk of developing the disease, have been identified. For example, being a carrier of a specific allele of the ApoE gene (ApoE4), which is involved in several neuronal protection mechanisms, increases the risk of developing the disease (by 3 to 15 times, depending on whether the patient is a carrier of one or two ApoE4 alleles). However, on its own, carrying this allele does not necessarily mean that you will develop the disease, as certain people who carry this allele will not develop the disease while other non-carriers will.
Certain environmental factors have been associated with Alzheimer’s disease. These include chronic sleep deprivation or taking certain psychotropic drugs such as benzodiazepines, which can increase the risk of developing the disease. A list of risk factors for Alzheimer’s disease was published recently, but the list is incomplete. Factors include excessive alcohol consumption, head injury, air pollution, low levels of education, high blood pressure, hearing problems, smoking, obesity, depression, physical inactivity, diabetes and social isolation.
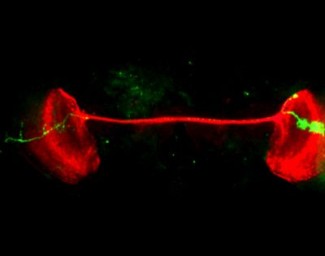
The degeneration of neurons that occurs in Alzheimer’s disease is the result of the concomitant progression of two types of lesion: the abnormal accumulation of ß-amyloid peptides (or A-beta peptides or Aß peptides) on the outside of cells, leading to the formation of ‘amyloid plaques’, also known as ‘senile plaques’; and the abnormal accumulation of the tau protein in neurons, leading to their degeneration.
Symptoms and diagnosis of Alzheimer’s disease
Memory loss is often the first symptom of Alzheimer’s disease, and this helps to guide diagnosis. This is followed by executive function disorders and temporo-spatial orientation problems, followed gradually by problems with language (aphasia), writing (dysorthography), movement (apraxia), behaviour and mood (anxiety, depression, irritability). The fact that the patient is unaware of these health problems (anosognosia) and that it is their relatives who report problems is, in itself, a diagnostic criterion.
Diagnosis is clinical, and now involves high-performance diagnostic tests such as a full neuropsychological assessment of cognitive functions, imaging tests such as MRI and glucose PET scans that highlight the areas of the brain that are affected, and finally lumbar puncture, which is capable of showing the biological markers of the disease. In other words, the presence of abnormal deposits of amyloid protein and tau protein.
Treatments for Alzheimer’s disease
Treatments for Alzheimer’s disease aim to slow the progression of the disease and enable patients and those close to them to adapt to the impairments that they are experiencing. Treatment is therefore multi-disciplinary.
Unfortunately, there is not yet any treatment that directly tackles the causes and mechanisms of the disease. Two types of medication – acetylcholinesterase inhibitors and memantine – have been approved and are used worldwide. They strengthen the brain’s circuits and, in some cases, stabilise the clinical picture of the disease.
The team is interested in the molecular mechanisms involved in the initiation and progression of Alzheimer’s disease and prion diseases.
Read more
The ARAMIS team, led by Ninon BURGOS & Olivier COLLIOT, aims to build numerical models of brain diseases, particularly neurodegenerative pathologies, from multimodal patient databases. The main approaches used are machine learning (artificial...
Read more
The goal of the Frontlab team is to understand better the role and organization of the prefrontal cortex in the control, activation, and inhibition of goal-directed behaviours.
Read moreSupport Paris Brain Institute
Did you like this content and did it answer the questions you were asking? Don't hesitate to support Paris Brain Institute.