Obsessive-compulsive disorder (OCD) affects 2–3% of the population. Symptoms typically appear at around the age of 20 (or 14 in 25% of cases), with repeated, persistent, unwanted and often anxiety-provoking ideas or images. These obsessions are often accompanied by repetitive behaviours designed to neutralise the anxiety and anguish resulting from the obsessions, known as compulsions. OCD is considered to be a disease of behaviour, thought and emotion. Around a third of patients with OCD have also had – or still have – tics.
In severe cases of obsessive-compulsive disorder (OCD), some patients can spend several hours a day performing compulsive rituals, causing a major impairment in their daily, family, social or professional lives.
Biological mechanisms and causes of OCD
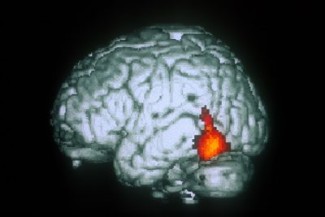
The causes of obsessive-compulsive disorder are unknown, although it is potentially linked to a non-hereditary genetic component. However, the brain regions involved in obsessions and compulsions have now been identified.
Using functional MRI or magnetoencephalography techniques, researchers have identified dysfunction in two distinct brain areas in the frontal lobe and the orbitofrontal and ventromedial prefrontal regions. Deeper areas of the cortex also play an essential role in these disorders, namely the basal ganglia.
OCD symptoms and diagnosis
The visible symptoms of obsessive-compulsive disorder, such as repetitive behaviours (compulsions) like frequent and excessive hand-washing, are merely the outward manifestation of the obsessions suffered by the patients, in this case an irrational fear of being infected by a virus or bacteria. These compulsions, or compulsive rituals, reflect an irrepressible need to alleviate or avoid the anxiety or anguish caused by the obsessions.
A large proportion of patients suffering from OCD have concomitant mental disorders. 75% of sufferers also have anxiety disorders, and 50–60% have severe depression or are diagnosed as bipolar. The risk of suicide is significantly higher in these patients.
In most cases, OCD is diagnosed based on clinical signs of obsession and/or compulsion that take up a significant amount of time in the patient’s day or which cause pathological distress and suffering.
Treatments for OCD
Patients are generally offered two effective treatments for OCD. First, there are ritual exposure and prevention psychotherapy sessions, which involve putting patients in a situation that generally triggers the obsession or compulsion, while preventing the obsession or compulsion from occurring. Over the course of the sessions, the patient gradually becomes aware of how the rituals are not helpful in reducing anxiety until the compulsive need for the ritual, which has been fairly constant over time (usually several years), disappears entirely.
The second effective therapy is drugs-based, by means of serotonergic antidepressants. A combination of the two strategies often offers the best treatment.
In more severe cases, deep brain stimulation via implanted electrodes may be the only effective therapeutic solution.
The objective of the team is to characterize the anatomy of the cortical region and the physiology of brain networks involved in motor control. The ultimate goal of this work is to develop new therapies and applications for deep brain stimulation.
Read moreSoutenez l'Institut du Cerveau
Ce contenu vous a plu et vous a permis de répondre aux questions que vous vous posiez ? N'hésitez pas à soutenir l'Institut du Cerveau.


