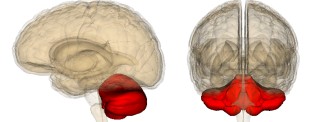
Ataxia, also known as cerebellar syndromes or motor coordination disorders, is caused by dysfunction of the cerebellum, a region of the brain that controls voluntary movement, balance and posture. The symptoms of Ataxia are directly related to the area of the cerebellum affected.
Causes of ataxia
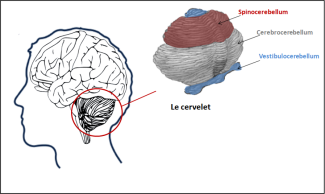
The cerebellum consists of 3 parts:
- The vestibulocerebellum (or archicerebellum) that controls balance and eye movements
- The spinocerebellum (or vermis) coordinates movements of the trunk and lower limbs such as posture and walking
- The cerebrocerebellum (or lateral hemispheres) that controls the precise and rapid movements of essentially the upper limbs.
There are three main types of cerebellar ataxia:
- Ataxia due to congenital malformations of the central nervous system, particularly the cerebellum. Symptoms appear in childhood and are not very progressive.
- Acquired ataxia resulting from brain damage, inflammation, or prolonged and recurrent exposure to toxic substances.
- Inherited ataxia due to genetic mutations that can be passed from generation to generation in a dominant or recessive fashion.
Acquired ataxia
These pathologies appear abruptly without evolution and are mostly due to damage of the cerebellum as a result of another disease or trauma.
Tumours, cysts, vascular disorders such as stroke or hematoma, and multiple sclerosis lesions if they are located in or near the cerebellum can cause symptoms of ataxia.
Similarly, an infection that affects the brain, such as HIV, prion disease and leukoencephalopathy, sometimes lead to the appearance of ataxia symptoms.
Patients with severe vitamin B12 or E deficiency, hyperthyroidism or hypothyroidism often have cerebellar disorders.
Long-term and recurrent exposure to toxic substances such as alcohol, lead and organic solvents may be responsible for the development of ataxia.
In inflammatory, metabolic, and toxic ataxia, there is a rapid progression of symptoms after a sudden onset that stops only after the cause has been removed.
Genetically Induced Cerebellar Ataxia
Autosomally dominant ataxia
These pathologies have an incidence of 1-5/100,000 persons. They include cerebellar and spinocerebral ataxia
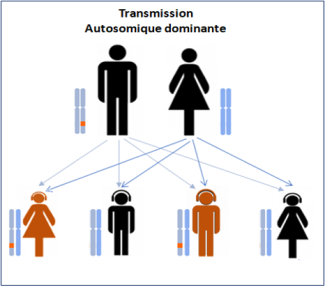
They appear on average around the age of 30 and are mainly due to genetic mutations, with at least 43 genes of the spino cerebellar ataxia (SCA) family located on different chromosomes.
In about 40% of patients, the gene responsible for ataxia symptoms has not yet been identified.
The most common type is spinocerebral ataxia type 3 with brain and spinal cord damage due to a mutation in the SCA3 gene (between 23 and 36% of family cases).
Autosomal recessive ataxia
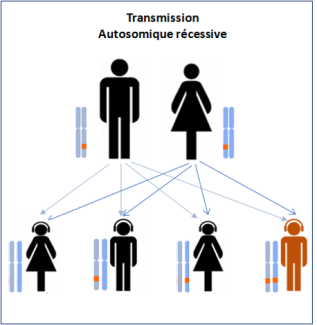
Autosomal recessive ataxia most often occurs before age 25, with some forms appearing before age 5.
Early onset ataxia, Friedreich ataxia, and telangiectatic ataxia are distinguished.
The ataxia of FRIEDREICH
This pathology affects about 1300 patients in France, with symptoms generally occurring between the ages of 7 and 14. This ataxia is due to mutations in the X25 gene, which encodes a protein called FRATAXINE that regulates the amount of iron in the mitochondria, a small structure essential for the survival of cells such as neurons.
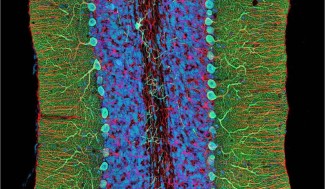
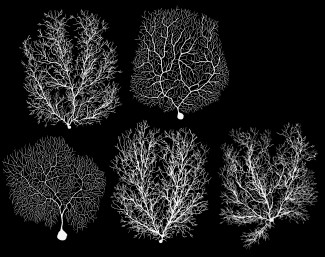
When frataxin is mutated, it accumulates in the mitochondria, leading to dysfunction of the cerebellum. In this pathology, the symptoms are essentially due to the death of neurons in areas of the spinal cord whose role is to inform the brain about the position of the body, about balance and about motor skills.
Telangiectatic ataxia
The gene responsible for this disease is called ATM. It codes for a protein that “repairs” DNA, the molecule that supports genetic information. In particular, its role is to prevent cell death.
This ataxia usually begins around 1 or 2 years of age. As with other ataxia, the symptoms observed are caused by an excess of neuronal death in the cerebellum, as neurons are unable to “repair” their DNA due to a lack of functional ATM protein.
The name telangiectasia comes from a particular symptom, observed in patients and specific to this pathology, the dilatation of small blood vessels at eye level, inside the ears, on the eyelids or at the level of the folds of the elbows and knees.
At Paris Brain Institute
Giovanni STEVANIN, INSERM/EPHE researcher and co-leader of the team “Fundamental and translational neurogenetics”
The “Fundamental and Translational Neurogenetics” team, co-led by Prof. Alexandra DURR and Giovanni STEVANIN, is working on Friedreich ataxia.
This team is identifying in particular a neuropsychological profile of patients with this ataxia.
And is participating in an international phase 2a therapeutic trial “FRAMES” to evaluate the efficacy and safety of MIN-102 in patients with Friedreich’s Ataxia.